Legg Calve Perthes Disease vs Slipped Capital Femoral Epiphysis
Legg Calve Perthes Disease (LCPD) A rare vascular femoral condition in children that affects the hip, this occurs when the blood supply to the rounded head of the femur(thigh bone) is temporarily disrupted causing vascular necrosis, a process in which bone cells die from lack of adequate blood supply.
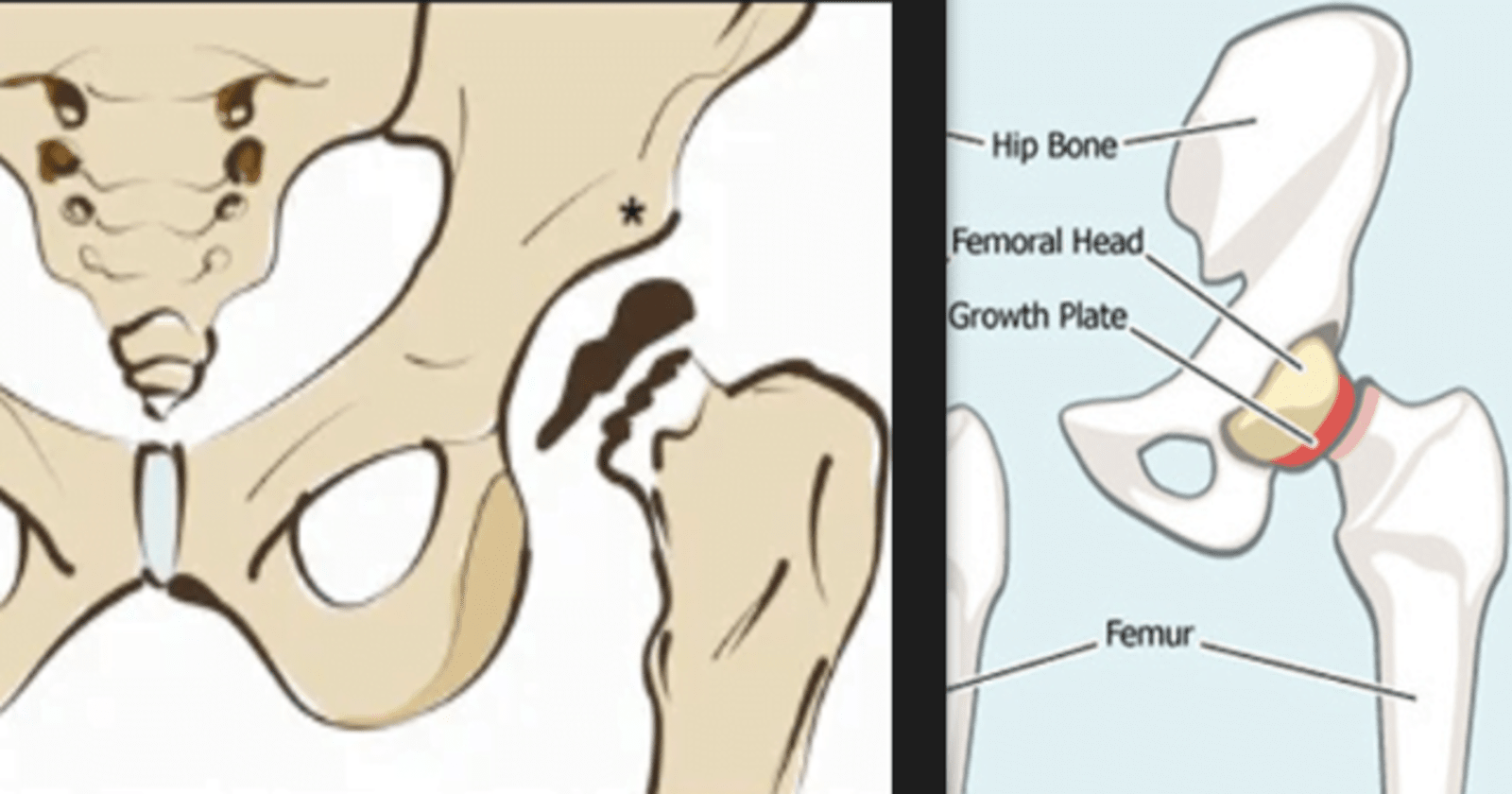
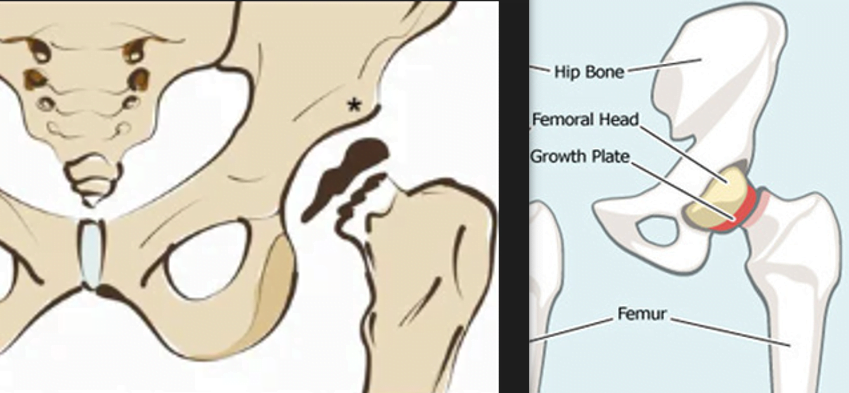
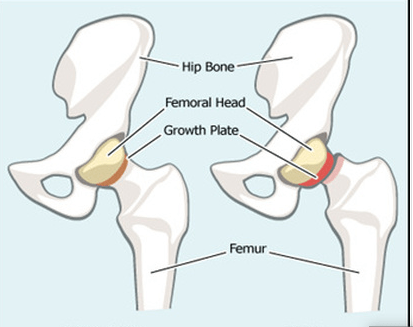
Slipped Capital Femoral Epiphysis (SCFE) is a condition that primarily affects adolescents during their growth spurt. It involves the displacement of the ball at the upper end of the thigh bone (femur) from the hip joint. Specifically, the epiphysis (the rounded end of the bone that forms part of the joint) slips off the neck of the femur through the growth plate. This displacement can occur in varying degrees, from a mild slip to a more severe slip.
The key differences between Legg-Calve-Perthes Disease (LCPD) and Slipped Capital Femoral Epiphysis (SCFE):
Legg-Calve-Perthes Disease (LCPD)
Slipped Capital Femoral Epiphysis (SCFE)
Avascular necrosis of the femoral head
Slip of the femoral head at the epiphysis
Typically 4 to 8 years old
Usually in pre-teens and early teens
More common in boys (4:1 male-to-female ratio)
More common in boys, especially during adolescence
Often unknown; may involve vascular or genetic factors
Multifactorial, involving factors like obesity, hormones, and genetics
Insidious hip pain, limping, reduced range of motion
Acute hip or knee pain, limping, decreased range of motion
Flattened or fragmented femoral head, joint space widening
Displacement of femoral epiphysis relative to femoral neck
Degenerative changes in the hip joint
Risk of avascular necrosis, deformity, and arthritis
Legg Calve Perthes Disease vs Slipped Capital Femoral Epiphysis
In Legg-Calve-Perthes (LEG-kahl-VAY-PER-tuz) disease when the blood flow to the femoral head, the ball-shaped part of the hip joint, is momentarily halted, the bone starts to undergo a process of temporary death. Over time, this weakened bone can fracture and lose its original round shape. Although the body eventually restores blood supply to the femoral head, facilitating the healing process, the reshaping of the ball may lead to persistent pain and stiffness. The entire sequence of bone degeneration, fracture, and regeneration can span several years.
Key Differences between Legg-Calve-Perthes Disease (LCPD) vs Slipped Capital Femoral Epiphysis (SCFE)
Legg-Calve-Perthes Disease (LCPD)
Slipped Capital Femoral Epiphysis (SCFE)
A vascular necrosis of the femoral head, leading to deformity and dysfunction.
Displacement of the femoral epiphysis from the metaphysis through the growth plate.
Typically occurs in children aged 4 to 10 years, with a peak incidence around 6 years old.
Primarily seen in adolescents during the pre-pubertal and early pubertal growth spurt, around 9 to 16 years old.
Usually affects one hip, but it can occur bilaterally in about 10-20% of cases.
Often affects only one hip, but bilateral cases can occur in about 20-40% of cases.
Gradual onset of hip pain, limping, and decreased range of motion.
Sudden or gradual onset of hip or knee pain, limping, and reduced range of motion.
Involve a disruption of blood supply to the femoral head.
Multifactorial, with obesity and hormonal changes playing a role. It may be related to increased stress on the growth plate.
X-rays show a flattened femoral head and joint space narrowing in later stages.
X-rays reveal a slip of the femoral epiphysis relative to the metaphysis.
Non-surgical options include activity modification, physical therapy, and bracing. Surgical options may include osteotomy or joint replacement in severe cases.
Surgical intervention is often necessary, involving stabilization of the slipped epiphysis with screws.
Prognosis varies, with a better outcome if diagnosed and treated early. Long-term outcomes may include hip arthritis.
Prognosis is generally good with early diagnosis and treatment. Untreated cases can lead to long-term complications, including hip arthritis.
5 key stages of Legg-Calvé-Perthes disease include:
Initial Stage (Necrosis):
Blood supply to the femoral head is disrupted, leading to bone cell death (necrosis).
This stage is often asymptomatic or may present with mild pain in the hip or groin.
Fragmentation Stage:
The necrotic bone gradually breaks into fragments, leading to the collapse of the femoral head.
Increased pain and stiffness may be experienced during this stage.
Revascularization Stage:
New blood vessels begin to grow into the dead bone, promoting healing.
The body attempts to revascularize and rebuild the femoral head.
Re-ossification Stage:
New bone forms in the shape of the femoral head.
The hip joint begins to remodel as the healing process continues.
Healed or Residual Deformity Stage:
The bone continues to remodel, and the femoral head regains its shape.
However, in some cases, there may be residual deformities or abnormalities in the hip joint.
The exact cause of Legg-Calvé-Perthes disease is not well understood, but it is believed to be related to a disruption in the blood flow to the femoral head. Possible contributing factors and risk factors include:
Genetics: There may be a genetic predisposition, as the disease sometimes runs in families.
Blood Supply Issues: Insufficient blood flow to the femoral head can occur, possibly due to blood vessel abnormalities.
Trauma: Some cases may be associated with trauma or injury to the hip.
Key Symptoms of Legg-Calvé-Perthes disease
The symptoms of Legg-Calvé-Perthes disease can vary, but common signs and symptoms include:
Limping: A noticeable limp is often one of the earliest signs of Perthes disease. Children may favor one leg over the other while walking.
Hip or groin pain: Children with Perthes disease may experience pain in the hip or groin area. This pain may be mild at first but can become more pronounced as the condition progresses.
Limited range of motion: There may be a decreased range of motion in the affected hip joint. Children may find it difficult to move their hip or may experience stiffness.
Muscle atrophy: As the disease progresses, muscle atrophy (wasting) may occur in the affected leg.
Shortening of the leg: Over time, the affected leg may appear shorter than the unaffected leg due to the collapse of the femoral head and the resulting deformity.
Joint stiffness: Stiffness in the hip joint can occur, making it challenging for the child to perform certain movements.
It’s important to note that the severity of symptoms can vary from one child to another, and the progression of the disease can also differ. If a child is experiencing persistent hip pain or difficulty walking, it is essential to consult a healthcare professional for a proper diagnosis and appropriate management. Early detection and intervention can improve outcomes for children with Legg-Calvé-Perthes disease. Treatment may involve various approaches, including physical therapy, bracing, and in some cases, surgery.
Dogs Affected by Legg-Calvé-Perthes disease
Legg-Perthes disease, also known as Legg-Calve-Perthes disease, aseptic necrosis of the femoral head, or avascular necrosis of the femoral head, is a condition that causes lameness in the hip joint of young, small breed dogs. Typically, toy breeds or terriers aged between five to eight months are commonly affected, although a range of small breeds up to a year old can also be susceptible.
The disease initiates with a disruption in the blood supply to the femoral head, which is the ball-shaped part of the hip joint. Consequently, portions of the bone tissue, deprived of their blood supply, undergo necrosis, leading to the collapse of the overlying cartilage that lines the hip joint. This results in a painful and poorly-fitting hip joint.
Initially, dogs with Legg-Perthes disease exhibit signs of pain and lameness. Some owners report that affected dogs may cry out when stretching the limb or attempting to bear weight. As the lameness persists and the dog begins to favor the affected leg, the muscles in the hip and thigh region may atrophy due to lack of use.
While Legg-Perthes disease typically affects only one hip, approximately one out of every six to eight cases may involve both hips. Early detection and appropriate veterinary intervention are crucial for managing this condition and alleviating the associated pain and discomfort in affected dogs.
Types/Breed of Dogs affected byLegg-Calvé-Perthes disease
Affenpinscher Australian terrier Bichon Frise Boston terrier Cairn terrier Chihuahua Cocker spaniel Dachshund Fox terrier Jack Russell terrier Lakeland Terrier Manchester terrier
small dog
Miniature pinscher Miniature schnauzer Pekingese Pomeranian Poodle Pug Schipperke Scottish terrier Shetland sheepdog Silky terrier Small breed Terriers Toy breeds Welsh terrier West highland white terrier
Simple Preventive Measures and Early Intervention of Legg-Calvé-Perthes Disease
Regular Pediatric Check-ups:
Routine pediatric check-ups can help in the early detection of any developmental issues or hip abnormalities. Early identification of risk factors or signs of Legg-Calvé-Perthes disease allows for timely intervention.
Healthy Lifestyle and Nutrition:
Promoting a healthy lifestyle, including proper nutrition and regular exercise, can contribute to overall skeletal health. Adequate calcium and vitamin D intake are essential for bone development and maintenance.
Avoidance of Smoking:
Maternal smoking during pregnancy has been linked to an increased risk of Legg-Calvé-Perthes disease. Encouraging expectant mothers to quit smoking may contribute to preventing the condition.
Physical Activity and Weight Management:
Regular physical activity and maintaining a healthy weight can reduce the risk of developing hip-related issues. Weight management is particularly important to minimize stress on the hip joint.
Genetic Counseling:
Legg-Calvé-Perthes disease may have a genetic component. Families with a history of the condition may benefit from genetic counseling to understand the potential risks and explore preventive measures.
Early Intervention
Early Diagnosis:
Early detection of Legg-Calvé-Perthes disease is critical for effective intervention. Pediatricians should be vigilant during routine check-ups, looking for signs and symptoms such as hip pain, limping, or limited range of motion.
Imaging Studies:
X-rays and other imaging studies are essential for confirming the diagnosis and assessing the extent of femoral head involvement. Early imaging allows healthcare professionals to plan appropriate treatment strategies.
Orthopedic Consultation:
Timely referral to an orthopedic specialist is crucial for formulating an appropriate treatment plan. Orthopedic experts can provide guidance on the best course of action based on the child’s age, the severity of the condition, and other individual factors.
Conservative Management:
In the early stages, conservative measures such as limiting weight-bearing activities and using braces or casts may be employed to reduce pressure on the affected hip joint and promote healing.
Surgical Intervention:
In some cases, surgical procedures may be necessary. Early intervention with surgery can help correct deformities, improve joint function, and prevent long-term complications.
Physical Therapy:
Physical therapy plays a crucial role in rehabilitation. Early initiation of physical therapy helps maintain joint mobility, strengthen muscles, and improve overall functional outcomes.
Slipped Capital Femoral Epiphysis (SCFE)
Slipped Capital Femoral Epiphysis (SCFE)is a condition where the ball at the head of the femur (thighbone) slips off the neck of the bone in a backward direction. This causes pain, stiffness, and instability in the affected hip. The condition usually develops gradually over time and are more common in boys than girls and is most prevalent during the period of rapid growth that occurs during puberty. The exact cause is not always clear, but factors such as obesity and hormonal changes during adolescence are believed to contribute. The condition is often associated with conditions like endocrine disorders, kidney disease, and metabolic disorders.
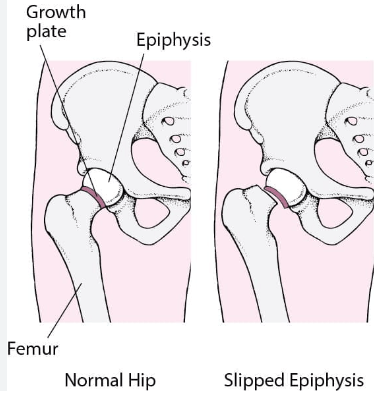
Normal hip joint vs SCFE
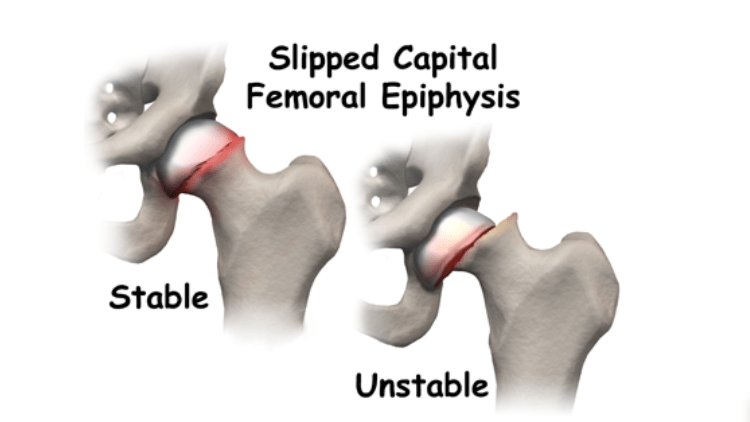
2 Types of Slipped Capital Femoral Epiphysis (SCFE)
There are two main types of slipped capital femoral epiphysis (SCFE)
Stable Slipped Capital Femoral EpiphysisSCFE: In cases of stable SCFE, the patient can bear weight on the affected hip, with or without the assistance of crutches. The majority of SCFE cases fall into this category.
Unstable Slipped Capital Femoral EpiphysisSCFE: This is a more serious form of slip where the patient is unable to put any weight on their hip, even with the support of crutches. Urgent treatment is necessary for unstable SCFE, as complications are more prevalent in these cases.
Stable Slipped Capital Femoral Epiphysis (SCFE)
Description: In stable SCFE, the femoral head has slipped, but the patient can still bear weight on the affected hip. The slip may be mild to moderate in nature.
Symptoms: Patients with stable SCFE may experience pain and discomfort in the hip or knee. However, they are generally able to walk and perform daily activities, possibly with the aid of crutches.
Diagnosis: Diagnosis is typically made through clinical examination, X-rays, and sometimes additional imaging studies. The degree of slippage is assessed to determine the stability of the condition.
Treatment: Management often involves surgical intervention to stabilize the hip joint and prevent further slippage. In some cases, conservative measures such as rest and physical therapy may be recommended.
2. Unstable Slipped Capital Femoral Epiphysis(SCFE)
Description: Unstable SCFE is a more severe form of slip where the femoral head has significantly displaced, making weight-bearing on the affected hip impossible, even with crutches.
Symptoms: Patients with unstable SCFE may experience intense pain and are unable to bear weight on the affected leg. There may be a noticeable change in the alignment of the leg.
Diagnosis: Urgent medical attention is required for diagnosis, involving imaging studies such as X-rays or possibly MRI to assess the severity of the slip and plan appropriate treatment.
Treatment: Urgent surgical intervention is typically necessary to stabilize the hip joint and prevent complications. The goal is to realign the femoral head and secure it in place to avoid further displacement.
Complications: Complications associated with SCFE, particularly in unstable slips, may include avascular necrosis (loss of blood supply to the femoral head), chondrolysis (damage to the cartilage), and early onset arthritis. Timely and appropriate treatment is crucial to minimize the risk of complications and optimize long-term outcomes.
Key Important Symptoms of Stable Slipped Capital Femoral Epiphysis (SCFE) vs Unstable (SCFE)
Stable SCFE
Intermittent Pain:
Pain in the groin, hip, knee, and/or thigh.
Worsening of pain with activity.
Altered Gait:
Limping while walking or running, particularly after physical activity.
Changed Positioning:
Holding the affected side in a position of increased external rotation.
Resulting in an out-toed gait (walking with the toes pointed outward).
X-ray image of SCFE
Unstable (SCFE)
Hip or Knee Pain: Persistent pain in the hip or knee is a common symptom of SCFE. The pain may be mild initially but can progress over time.
Limping: A noticeable limp or difficulty walking may be present, particularly if the pain is severe.
Limited Range of Motion: There may be a reduced range of motion in the hip joint, making certain movements uncomfortable or difficult.
External Rotation of Leg: The affected leg may turn outward, leading to an abnormal walking posture.
Discrepancy in Leg Length: One leg may appear shorter than the other due to the slippage of the femoral head.
Weakness in the Leg: Muscular weakness in the affected leg may occur
Symptoms of SCFE may include hip or knee pain, limping, and a limited range of motion in the affected hip. The condition is typically diagnosed through imaging studies, such as X-rays.
Treatment usually involves surgical intervention to stabilize the affected hip joint and prevent further slipping. The surgical options may include placing screws or pins to hold the bone in place. Physical therapy may also be recommended to aid in rehabilitation.
SCFE requires prompt diagnosis and treatment because if left untreated, it can lead to complications such as avascular necrosis, where the blood supply to the femoral head is compromised, resulting in damage to the bone tissue. Early intervention improves the prognosis and helps prevent long-term complications. If you suspect SCFE or if there are symptoms like hip or knee pain in an adolescent, it is important to seek medical attention for a thorough evaluation.
Treatment for Legg-Calve-Perthes Disease (LCPD) vs Slipped Capital Femoral Epiphysis (SCFE)
The treatment for Legg-Calve-Perthes Disease (LCPD) and Slipped Capital Femoral Epiphysis (SCFE) may vary based on the severity of the condition, the age of the patient, and other individual factors. Here’s an overview of the treatment approaches for each:
Basic interventions for Legg-Calve-Perthes Disease (LCPD):
Conservative Management:
Rest and Activity Modification: Limiting activities that put stress on the affected hip joint.
Physical Therapy: Exercises to maintain range of motion and strengthen muscles around the hip.
Containment Strategies:
Bracing: Sometimes, a brace or cast may be used to help contain and support the hip joint.
Surgical Intervention (in severe cases):
Osteotomy: Surgical procedures may be considered to reposition the femoral head or realign the hip joint.
Follow-up Care:
Regular monitoring with X-rays and clinical assessments to track the progress.
Long-term follow-up to address any potential complications.
Slipped Capital Femoral Epiphysis (SCFE)
Surgical Intervention:
In Situ Pinning: This involves stabilizing the slipped epiphysis with the use of screws.
Osteotomy: In some cases, a surgical realignment of the hip may be necessary.
Post-operative Physical Therapy:
Rehabilitation exercises to restore strength, flexibility, and function.
Gradual return to weight-bearing activities.
Activity Modification:
Limiting certain activities that may put stress on the hip joint.
Monitoring for Complications:
Regular follow-up appointments and imaging studies to monitor for complications, such as avascular necrosis (AVN).
Management of Underlying Conditions (if present):
Addressing any underlying factors contributing to SCFE, such as obesity or hormonal issues.
It’s important to note that early detection and intervention can significantly impact the outcomes for both conditions. The specific treatment plan will be determined by the orthopedic specialist based on the individual characteristics of the patient and the stage/severity of the disease. Patients with LCPD and SCFE may require ongoing monitoring and follow-up care into adulthood. Consultation with a healthcare professional is crucial for personalized advice and management.
Table comparing the Differences in diagnosis and treatment of Legg-Calve-Perthes Disease (LCPD) vs Slipped Capital Femoral Epiphysis (SCFE):
Legg-Calve-Perthes Disease (LCPD)
Slipped Capital Femoral Epiphysis (SCFE)
Diagnosis – Clinical examination
Diagnosis – Clinical examination
– X-rays of the hip joint
– X-rays of the hip joint
– MRI may be used for early detection
– MRI may be used for early detection
Symptoms – Pain in the hip, groin, or knee
Symptoms – Pain in the hip, groin, or knee
– Limping during walking
– Limping during walking
– Limited range of motion in the hip
– Limited range of motion in the hip
– Atrophy of thigh muscles
– Reduced internal rotation of the hip
Etiology – Idiopathic (unknown cause)
Etiology – Often associated with obesity and hormonal changes
Treatment – Conservative management:
Treatment – Surgical intervention may be required:
– Rest and activity modification
– Stabilization of the slipped epiphysis
– Physical therapy
– Surgery to prevent further slipping
– Containment strategies
– In situ pinning (screws) or other surgical methods
– If severe, surgical intervention may be needed
– Post-operative physical therapy for rehabilitation
Prognosis – Good prognosis with early diagnosis and treatment
Prognosis – Variable outcomes, may depend on severity and delay
– Potential long-term effects in some cases
– Risk of avascular necrosis (AVN) and hip arthritis
Comparison table
3 important Management and treatment strategies of Slipped Capital Femoral Epiphysis
Surgery:
Objective: The primary goal of surgery is to stabilize the slipped epiphysis and prevent further displacement.
Method: This is typically achieved by using screws to secure the femoral head (ball) to the femoral neck.
Importance: Surgical intervention is crucial to avoid complications and ensure proper healing.
Physical Therapy:
Objective: Physical therapy plays a vital role in the rehabilitation process post-surgery.
Focus areas: Therapeutic exercises aim to improve strength, flexibility, and overall function of the hip joint.
Benefits: Physical therapy helps restore normal range of motion, enhance muscle strength, and promote a faster recovery.
animation of a kid in the health care facility with nurse
3. Weight Management:
Rationale: Addressing obesity is essential in the management of SCFE.
Reasoning: Excess body weight can contribute to the development and recurrence of SCFE. It places additional stress on the hip joint and may exacerbate the condition.
Interventions: Weight management strategies may include dietary changes, regular exercise, and lifestyle modifications to achieve and maintain a healthy weight.
Resources
Some of my knowledge comes from my work experiences in the Operating room. Working along with Orthopedic surgeons and patients with these conditions.